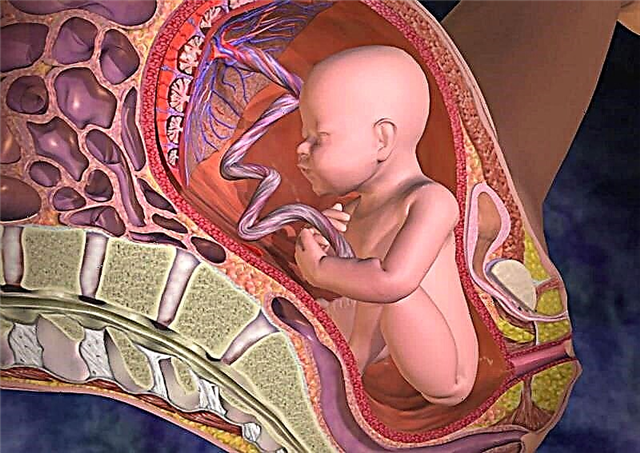
The structure and function of the heart in the fetus differ from the functioning of this organ in children after birth and in adults. First of all, the fact that in the heart of the baby residing in the mother's womb there are additional holes and ducts. One of them is the ductus arteriosus, which should normally close after childbirth, but this does not happen in some babies.

What is patent ductus arteriosus in children
The arterial or Botallovy duct is a vessel present in the heart of the fetus. The diameter of such a vessel can be from 2 to 10 mm and the length from 4 to 12 mm. Its function is to link the pulmonary artery to the aorta. This is required to carry blood around the lungs as they do not function during fetal development.
The duct closes when the baby is born, transforming into a cord that is impenetrable for blood, consisting of connective tissue. In some cases, the closure of the duct does not occur, and this pathology is called an open arterial duct, or abbreviated as PDA. It is diagnosed in one out of 2,000 newborns, while it occurs in almost half of premature babies. According to statistics, girls have this defect twice as often.
An example of what a PDA looks like on an ultrasound scan can be seen in the following video.
When should it close?
In most babies, the closure of the duct between the pulmonary artery and the aorta occurs in the first 2 days of life. If the baby is premature, the normal closure of the duct is considered to be up to eight weeks. The diagnosis of PDA is given to children in whom the Botallov duct remained open after reaching 3 months of age.

Why does not all newborns close?
A pathology such as PDA is quite often diagnosed with prematurity, but the exact reasons that the duct remains open have not yet been identified. The provoking factors include:
- Heredity.
- Low weight of the newborn (less than 2500 g).
- The presence of other heart defects.
- Hypoxia during intrauterine development and during childbirth.
- Down syndrome and other chromosomal abnormalities.
- The mother has diabetes.
- Rubella in a woman during gestation.
- Radiation exposure to a pregnant woman.
- The use of alcoholic beverages or substances with narcotic effects by the expectant mother.
- Taking medicines that negatively affect the fetus.
Hemodynamics in PDA
If the duct does not overgrow, then due to the higher pressure in the aorta, blood from this large vessel through the PDA enters the pulmonary artery, joining the blood volume from the right ventricle. As a result, more blood enters the vessels of the lungs, which causes an increase in the load on the pulmonary circulation, as well as on the right parts of the heart.

Phases
There are three phases in the development of PDA clinical manifestations:
- Primary adaptation. This stage is observed in children in the first years of life and is characterized by a pronounced clinic, depending on the size of the unclosed duct.
- Relative compensation. At this stage, the pressure in the pulmonary vessels decreases, and in the cavity of the right ventricle - increases. The result will be a functional overload of the right side of the heart. This phase is observed at the age of 3-20 years.
- Sclerosis of the pulmonary vessels. At this stage, pulmonary hypertension develops.
Signs
In babies of the first year of life, PDA is manifested:
- Increased heart rate.
- Shortness of breath.
- Small weight gain.
- Pallor of the skin.
- Sweating.
- Increased fatigue.
The severity of the manifestation of the defect is influenced by the diameter of the duct. If it is small, the disease can proceed without any symptoms. When the vessel size is more than 9 mm in term babies and more than 1.5 mm in premature babies, the symptoms are more pronounced. They are joined by:
- Cough.
- Hoarseness of voice.
- Frequent bronchitis and pneumonia.
- Development lag.
- Weight loss.

If the pathology was not detected until a year, then older children have the following signs of PDA:
- Breathing problems with little physical activity (increased frequency, feeling short of breath).
- Frequent infections of the respiratory system.
- Cyanosis of the skin of the legs.
- Underweight for your age.
- The rapid appearance of fatigue during outdoor games.
The danger
When the Botallic duct is not closed, blood from the aorta enters the vessels of the lungs and overloads them. This threatens the gradual development of pulmonary hypertension, heart wear and tear and a decrease in life expectancy.
In addition to the negative effect on the lungs, the presence of a PDA increases the risk of complications such as:
- Aortic rupture is a life-threatening condition.
- Endocarditis is a bacterial disease that affects the valves.
- A heart attack is the death of a part of the heart muscle.
If the diameter of the open duct is significant and there is no treatment, the child begins to develop heart failure. It manifests itself as shortness of breath, rapid breathing, high pulse, decreased blood pressure. This condition requires immediate hospital treatment.

Diagnostics
To identify a PDA in a child, use:
- Auscultation - the doctor listens to the baby's heartbeat through the chest, detecting murmurs.
- Ultrasound - this method detects an open duct, and if the study is supplemented by a Doppler, then it is able to determine the volume and direction of blood that is discharged through the PDA.
- X-ray - such a study will determine changes in the lungs, as well as cardiac boundaries.
- ECG - the results will reveal an increased load on the left ventricle.
- Probing the chambers of the heart and blood vessels - this examination determines the presence of an open duct using contrast, and also measures pressure.
- Computed tomography is the most accurate method and is often used before surgery.
Treatment
The doctor determines the tactics of treatment, taking into account the symptoms of the defect, the diameter of the duct, the age of the child, the presence of complications and other pathologies. Therapy for PDA can be medical and surgical.

Conservative treatment
They resort to it with unexpressed clinical manifestations of the defect and the absence of complications. As a rule, the treatment of babies in whom a PDA is detected immediately after childbirth is first medication. The child may be given anti-inflammatory drugs such as ibuprofen or indomethacin. They are most effective during the first months after birth because they block substances that prevent the duct from closing naturally.
Diuretics and cardiac glycosides are also prescribed to reduce the stress on the heart.
Operation
Such treatment is the most reliable and is:
- Duct catheterization. This treatment is often used over 12 months of age. It is a safe and fairly effective manipulation, the essence of which is the introduction of a catheter into a large artery of a child, which is fed to the PDA, in order to install an occluder (a device for blocking the blood flow) inside the duct.
- Ligation of the duct during open surgery. This treatment is often given between 2 and 5 years of age. Instead of bandaging, it is possible to suture the duct or clamp the vessel using a special clip.

All these terms sound a little scary, but in order not to be afraid, you need to know what exactly will be done to your child and how it will happen. In the following video, you can see how the occluder is installed in the duct in practice.
Indications for surgical intervention with PDA are the following situations:
- Drug therapy was ineffective.
- The child has symptoms of blood congestion in the lungs, and the pressure in the pulmonary vessels has increased.
- The child often suffers from pneumonia or bronchitis, which is difficult to treat.
- The child has developed heart failure.
The operation is not prescribed for severe kidney or liver disease, as well as in a situation where blood is thrown not from the aorta, but into the aorta, which is a sign of serious damage to the pulmonary vessels that cannot be corrected surgically.
Forecast
If the Botallov duct did not close in the first 3 months, in the future it happens on its own very rarely. A child born with a PDA is prescribed drug therapy to stimulate the clotting of the duct, which is 1-3 courses of injections of anti-inflammatory drugs. In 70-80% of cases, such medications help to eliminate the problem. If they are ineffective, surgical treatment is recommended.
The operation helps to completely eliminate the defect itself, facilitate breathing and restore lung function. Mortality during surgery for PDA is up to 3% (in full-term babies, there are almost no lethal cases), and in 0.1% of operated babies, the duct reopens after a few years.

Without treatment, few children born with a major PDA survive to more than 40 years of age. Most often, they develop pulmonary hypertension from the second or third year of life, which is irreversible. In addition, the risk of endocarditis and other complications increases. While surgical treatment provides a favorable outcome in 98% of cases.
Prevention
To reduce the risk of a baby with a PDA, it is important to:
- For the period of pregnancy, give up alcoholic beverages and smoking.
- Do not take medications not prescribed by a doctor during gestation.
- Take protective measures against infectious diseases.
- In the presence of heart defects in the family, consult a geneticist before conception.