
Respiratory disorders, in which bronchial conduction is disturbed, leads to the development of broncho-obstructive syndrome. With prolonged course, this condition turns into asthma.


What it is?
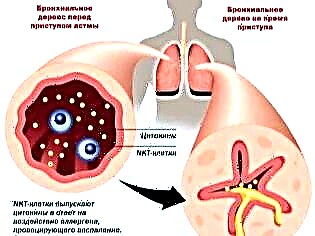
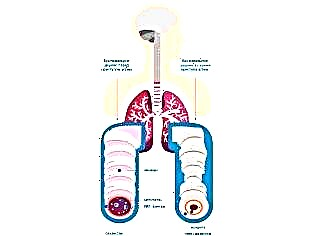
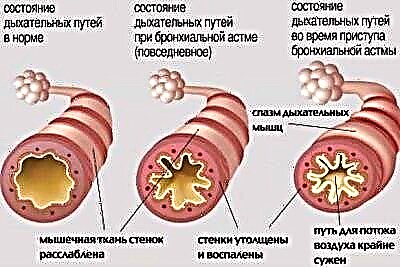
Several different reasons lead to the development of respiratory disorders. In bronchial asthma, there is an increased reactivity of the bronchi to certain substances, which leads to the development of bronchial obstruction (blockage). Air with oxygen dissolved in it does not pass well through the narrowed bronchi. As a result, this leads to disturbances in air exchange between blood, lung tissue and the environment.

After exposure to various provoking factors, a violation of bronchial conduction occurs. This condition is called broncho-obstructive syndrome. If this process lasts a long time, then the course of the disease becomes chronic. In this case, the broncho-obstructive syndrome becomes bronchial asthma.
According to statistics, this disease occurs in 10% of children. Boys get sick more often than girls. The peak incidence occurs at the age of 4-10 years.
Bronchial asthma is found not only in pediatrics. Adults can also get sick. The first signs of the disease can occur at any age.
The course of bronchial asthma is undulating. The periods of exacerbations are followed by remissions. The length of the quiet period may vary. It depends mainly on the state of the immune system and the presence of concomitant chronic diseases in the child. Weakened toddlers have far more exacerbations than children who undergo regular rehabilitation.
Risk factors
Various provocateurs can lead to the development of bronchial asthma. In some situations, the action of several provoking factors at once has a more pronounced effect, leading to persistent broncho-obstructive syndrome.

Among the most significant risk factors:
- Genetic predisposition. If one of the parents has bronchial asthma, then the risk of having a sick baby is 25%. In cases where dad and mom are both sick, the risk of a child with respiratory failure is already 75%. Not in all cases, a genetic predisposition leads to the development of the disease. If the child is not affected by other adverse factors, then he may not develop the disease throughout his life.
- Contaminated air. Children who live near industrial plants and factories, as well as near major highways, have a higher risk of developing bronchial asthma. The smallest particles of toxic products can remain in the air for a long time. When in contact with the mucous membranes of the upper respiratory tract, they easily cause inflammation, leading to bronchial obstruction.

- Dust and mites that live in pillows and blankets. These seemingly harmless factors often lead to the development of persistent symptoms of bronchial obstruction. The smallest mites are constantly in contact with the skin, causing severe allergies. Ultimately, this leads to severe breathing problems.
- Animals. The most dangerous are pets that live at home. Wool, fluff, and animal dander often become a source of severe allergic reactions. It manifests itself not only by the appearance of specific rashes on the skin, but also characterized by the presence of impaired breathing.


- Food products. Especially industrially prepared food. There are a lot of synthetic additives, dyes and aromatic components in such products. Once in the gastrointestinal tract, they cause severe allergic reactions. This contributes to the development of systemic adverse symptoms: coughing up sputum and wheezing when breathing.

- Household chemicals. Many synthetic products contain a fair amount of various perfume additives and fragrances. They have a pronounced irritant effect on the respiratory tract. With prolonged contact with such products, the risk of developing bronchial obstruction in a child increases many times.
- Individual sensitivity to herbal bloom. Usually attacks of bronchial asthma in this condition have a clear seasonality. The baby's well-being worsens in spring and autumn. It was at this time that weeds and meadow grasses, as well as various trees and shrubs, bloom.
- Strong humidity and dampness in the room. This condition provokes the development of molds. In wet and damp conditions, they grow and multiply rapidly. Large colonies of mold fungi can cause severe breathing problems in your baby.
- Infection with viruses and bacteria. Currently, more and more doctors began to register the virus-induced form of bronchial asthma. In a frequently ill child with reduced immunity, the development of broncho-obstructive syndrome often becomes a consequence of a viral infection. Also, in some cases, and bacterial infections lead to asthmatic breathing disorders.

- Ingestion of tobacco smoke. The influence of passive smoking on the development of bronchial asthma has been scientifically proven. If one of the parents constantly smokes in the apartment or room where the child is, then the risk of developing bronchial asthma increases significantly.
- Strong physical exertion, leading to exhaustion. Excessive training, chosen incorrectly, can lead to impaired functioning of the immune system. After prolonged stress, the child develops breathing problems and shortness of breath.
Causes of occurrence
Bronchial asthma most often develops when the child has a genetic predisposition initially. With the additional influence of unfavorable environmental factors, the course of the disease worsens and the transition to a chronic form occurs.

The development of asthmatic breathing disorders is caused by:
- Eating hyperallergenic foods. Most often these are: citrus fruits, chocolate, sweets, seafood, fish, honey and others. The ingestion of allergenic products into the body leads to the development of an allergic reaction. It can manifest itself in particular and a pronounced syndrome of bronchial obstruction.
- Inhalation of contaminated air. Toxic industrial products and exhaust fumes have toxic effects on the epithelial cells of the upper respiratory tract. These substances cause severe spasm of the bronchi, which leads to a narrowing of their lumen and impaired breathing.
- Allergic diseases. Often these pathologies are secondary and develop in the background with concomitant chronic diseases. The development of bronchial asthma is caused by: persistent dysbiosis, pathologies of the gastrointestinal tract, gallbladder dyskinesia and chronic hepatitis.
- Use of medicines without the prior recommendation of a doctor or selected incorrectly. All medications can have side effects. Many of them are capable of causing persistent bronchial obstruction. If the child has a genetic predisposition to bronchial asthma, this can lead to the development of the disease.
- Severe traumatic situation or stress. Cases of the development of the disease after moving to a new place of residence, divorce of parents, as well as death of close relatives in early childhood have been noted. Severe stress promotes the production of increased amounts of hormones. They cause narrowing of the bronchi, which leads to impaired breathing.
- Improper therapy for chronic respiratory diseases. Frequent bronchitis, especially those with a pronounced broncho-obstructive component, ultimately lead to the development of bronchial asthma. If a child often has a cough and has a cold up to 4-5 times a year, then parents should think about whether the baby has bronchial asthma.


Classification
All forms of allergic asthma can be divided into several groups. This classification is based on the causes that cause the disease. This distinction is very important in pediatric pulmonology. This classification helps doctors prescribe the right treatment.
Given the leading cause, bronchial asthma can be:

- Allergic. The development of this form of the disease leads to the ingress of allergens into the body, provoking the development of unfavorable systemic manifestations. In the presence of individual hypersensitivity to foreign substances in the baby, the level of immunoglobulins E increases. These components lead to a pronounced spasm of the bronchi, which is manifested by the appearance of a cough.
- Non-atopic. In this form of the disease, spasm in the bronchi occurs due to any exposure, but not an allergen. This type of asthma develops as a result of severe stress, hypothermia, or as a result of excessive and improperly selected physical activity.
- Mixed. May occur as a result of exposure to both allergic and non-atopic causes. It is characterized by the appearance of numerous symptoms. The course of the disease is usually the most calm. The periods of remission can be quite long.
- Status asthmaticus. This highly dangerous medical emergency stands out as a distinct form of bronchial asthma. Over the course of a child's life, several of these seizures may occur. This condition is extremely serious, in which the symptoms of respiratory failure sharply increase. In this case, urgent treatment is required.

The course of bronchial asthma can be different. This is influenced by several factors at once:
- the age at which the baby has the first signs of the disease;
- state of immunity;
- the presence of concomitant chronic diseases;
- region of residence;
- the adequacy of the selected treatment.

All forms of the disease can be divided into several groups, taking into account the features of the severity:
- With a slight episodic course. With this form, the functions of external respiration are not noted. Disturbed breathing attacks occur less frequently than once a week. The seizure-free period can be quite long.
- With a slight persistent course. It is characterized by the appearance of attacks of disturbed breathing several times during the week. There is no daily deterioration in well-being. When an attack occurs, breathing is disturbed, a harsh cough appears, and shortness of breath increases. Spirometry does not show any abnormalities.
- With a moderate course. Deterioration in well-being occurs almost every day. During such attacks, the child's sleep is disturbed, and there is also severe breathing disorders, leading to severe shortness of breath. In the treatment of the condition, the daily use of bronchodilators is required. Spirometry shows deviations from the norm by 20-40%.
- With a heavy course. They are dangerous by the development of several attacks in one day. Also, such deterioration can occur at night. Therapy with short-acting bronchodilators does not bring a pronounced effect. To control the course of the disease, hormones are required. Spirometry shows a deviation from normal breathing parameters by more than 40%.
What is bronchial asthma in children, Dr. Komarovsky will tell in detail in the next video.
Symptoms
It is quite difficult to recognize bronchial asthma at the initial stage. Quite often, parents believe that the child has just an allergy or broncho-obstructive bronchitis. In the interictal period, sometimes even an experienced doctor often cannot determine asthma in a child. Further development of the disease is manifested by the development of characteristic adverse symptoms, which should alert parents.
For bronchial asthma during an exacerbation, it is characteristic:
- Shortness of breath. It is expiratory in nature. In this case, exhalation is noticeably difficult. You can check for shortness of breath at home on your own. This is evidenced by an increase in the number of respiratory movements per minute by more than 10% of the age norm.
- Cough with difficult expectoration. Mostly this symptom worries the child during the day. At night, the cough decreases somewhat. Sputum in bronchial asthma is rather viscous, "glassy". When trying to cough it up, the child may even develop soreness in the chest.
- Increased heart rate. Even in the absence of physical activity, the child develops tachycardia. This symptom is usually associated with shortness of breath. The more pronounced it is, the more the number of heartbeats increases in one minute.
- Dry wheezing on breathing. In severe cases, such breathing sounds become audible from the side, without the use of a phonendoscope. Wheezing - mostly dry and wheezing. It is believed that in bronchial asthma "an accordion plays in the chest."
- The appearance of a boxed sound during percussion. This method is performed to clarify the diagnosis. When tapping fingers on the chest, a characteristic sound is heard, reminiscent of striking an empty box. The appearance of this symptom manifests itself already in the distant stages of the disease and indicates an increased filling of the lungs with air.
- Lack of effect from conventional drugs, used to eliminate cough. Only bronchodilators and hormonal agents have a visible therapeutic effect. With an allergic form of bronchial asthma, antihistamines have a pronounced effect.

Symptoms of an attack
- The well-being of the child during the worsening of the disease is greatly disturbed. The kid becomes more moody, frightened. Some babies, especially in the first months after birth, begin to cry, they ask for more hands. Babies almost completely lose their appetite, they refuse to eat.
- During an attack, the child has increased expiratory dyspnea. To alleviate this condition, the baby often takes a forced position. He leans forward strongly. The head may be slightly thrown back.
- Often asthmatic babies during an attack try to put their hands on a chair or even a bed rail. Such a forced position somewhat facilitates the discharge of sputum and improves breathing.
- With a severe attack the baby shows symptoms of respiratory failure. The lips become pale and, in some cases, even bluish. Hands and feet are cold to the touch. The child has a paradoxical pulse. With this rhythm disturbance, the number of heart contractions changes during inhalation and exhalation.
- Some babies try to take a sitting position. This helps them breathe better. Even from the outside, the participation of the auxiliary respiratory muscles in breathing is visible. The child breathes deeply and quickly. The condition is aggravated by a violent hacking cough. In some cases, it even leads to the fact that the child begins to cry.
- After the attack, the baby feels overwhelmed. Some children cannot calm down for a long time. Their sleep is disturbed. The duration of the attack may vary. With late use of inhalers, a dangerous and life-threatening condition can develop - status asthmaticus. In this situation, it is impossible to cope with the elimination of adverse symptoms at home - an ambulance is required.

How does it manifest in infants?
The course of bronchial asthma in an infant can also proceed in different ways: from mild severity to the most severe. Infants often have asthma attacks on fermented milk products and molds. Food allergies are the second most common.
Usually, the first symptoms of bronchial asthma in an infant appear by the age of 5-6 months. At this time, the baby begins to receive new food products as complementary foods. If a child has an individual intolerance or hypersensitivity to a substance, he may develop symptoms of bronchial obstruction.
A striking symptom of bronchial asthma in an infant is the onset of cough. The kid begins to cough both day and night. In some cases, shortness of breath joins. Even while in bed, without physical activity, the child's breathing and heart rate increase in one minute.
Babies begin to suck poorly, the effectiveness of breastfeeding decreases. Such children lose weight and are somewhat behind their peers in terms of physical development. Silent crying is also one of the symptoms of bronchial asthma in a baby's first year of life. The child becomes lethargic, badly asks for hands. Some babies do not fall asleep well and often wake up during the night.


Diagnostics
In order to make the correct diagnosis, just taking anamnesis and examining the child by a doctor will not be enough. To identify persistent bronchial obstruction, additional tests and examinations are required. Only carrying out various diagnostic tests will help establish the correct diagnosis.


To diagnose bronchial asthma, you will need:
- General blood analysis. An increase in leukocytes and moderate eosinophilia (an increase in the number of eosinophils in the leukocyte formula) indicate increased allergization. Such changes are characteristic mainly for the allergic form of bronchial asthma.

- Sputum examination. The detection of specific Charcot-Leiden crystals, Kurshman coils, an increase in the number of desquamated epithelial cells, as well as an increased level of eosinophils indicate the presence of persistent bronchial obstruction.
- Conducting a study on the ratio of blood gases. With a prolonged course of bronchial asthma, there is a decrease in the content of dissolved oxygen and a slight increase in carbon dioxide. Such changes indicate the presence in the body of pronounced hypoxia or oxygen starvation of cells.
- Spirometry. Reflects indicators of external respiration. Evaluation of forced expiration and general indicators of vital capacity of the lungs helps to identify persistent bronchial obstruction in the body, leading to a change in the parameters of the respiratory function of the lungs. The decrease in these parameters is estimated as a percentage of the age norm.
- Carrying out scarification tests. They help identify all possible allergens that cause bronchial obstruction in a child. The study is carried out only by an allergist. The test is only possible for babies over five years old.
- Chest x-ray. It helps to establish the secondary signs of bronchial obstruction: increased airiness of the lungs and a change in the diameter of large bronchi.
- Bronchoscopy. It is used in limited cases, mainly for differential diagnostics in order to exclude similar diseases that occur, like bronchial asthma with symptoms of bronchial obstruction.

Complications
The development of adverse effects of bronchial asthma depends on many factors. The most important of them is timely diagnostics and correctly prescribed treatment. With an inadequately selected therapy regimen, a child may experience numerous adverse consequences of the disease.
Among the most frequently reported complications in bronchial asthma:
- Development status asthmaticus.
- Sudden onset of symptoms acute respiratory failure.
- Spontaneous pneumothorax... In this condition, a rupture of the capsule that covers the outside of the lungs occurs. This condition usually occurs during a severe attack.
- Build up shock... The development of acute respiratory failure leads to a sharp drop in blood pressure. This condition is extremely unfavorable and requires urgent treatment and hospitalization in a hospital.
- Pneumonia... It appears when the bacterial flora joins the inflammatory process. It is characterized by a rather severe course. Antibiotics are required to eliminate symptoms.
- Emphysema of the lungs... Develops in asthmatics with experience. It is characterized by increased air filling of the lung tissue. At the same time, the respiratory function of the lungs is significantly reduced, which leads to the appearance of symptoms of respiratory failure.
- Formation of cardiovascular failure... It is an extremely unfavorable complication. This condition requires the appointment of several types of drugs at once, including cardiac glycosides.

Treatment
According to clinical guidelines for the treatment of asthma, therapy for different forms of the disease should be stepwise. Modern medical standards provide for the gradual prescription of drugs.
The selection of the necessary drugs is carried out only after a comprehensive examination of the child. Before choosing the necessary inhalers or tablets, you should accurately identify the form of bronchial asthma and determine the severity of the disease.
A child with bronchial asthma is treated by a pulmonologist. In case of an allergic form, a child must be shown to an allergist. This doctor can help you design a more personalized treatment based on your immune system.
Treatment in a pulmonary clinic is carried out only in difficult cases. With a mild course, regular visits to the clinic and outpatient consultations with doctors are quite enough.
Treatment of bronchial asthma includes several basic principles:


- Appointment of symptomatic remedies. In this case, drugs are used only during an attack in order to eliminate the acutely emerging adverse symptoms of the disease. Typically, various inhalers are used for these purposes.

- Selection of basic therapy. These funds are already assigned for permanent admission. They help prevent new attacks and improve the course of the disease. The control of the effectiveness of drugs is carried out using spirometry. At home, a special portable device - a peak flow meter - is perfect for this purpose.
- Elimination of all types of allergens from everyday life. Compliance with a hypoallergenic diet, the use of special bedding, and restrictions on playing with soft toys will help prevent new attacks and the development of asthmaticus.
- Use of special humidifiers. These devices help to create an optimal indoor climate. Too dry air irritates the respiratory tract, causing respiratory problems and new asthma attacks.

- The use of antitussive and expectorant drugs. These funds help to eliminate a pronounced hacking cough. In the absence of allergies in the child, medicinal herbs are also suitable: mother and stepmother, thyme, calendula and others. Herbal medicine should be used only after consulting a doctor.
- Restricting games with animals. For a toddler suffering from bronchial asthma, it is best not to make furry friends at home. Animal hair and fluff can adversely affect the child's health and cause new seizures.


- Regular disinfection treatment. The child's visit should be cleaned daily. Do not use caustic and too aggressive chemicals for this. It is better to choose detergents that do not contain pronounced aromatic additives. The best option is household chemical products with special safety markings even in children's rooms.

- Strengthening the immune system. For this, active walks in the fresh air, exercise therapy complexes, breathing exercises, as well as various hardening are perfect. The child should be properly tempered from the earliest years of his life. Tempering should be regular. The complex of these measures will help to strengthen the weakened immunity of the baby, which will help to reduce asthma attacks in the future.
Drug therapy
Various groups of drugs are used as basic treatment. Among them:
- Mast cell membrane stabilizers. Helps to reduce the amount of pro-inflammatory biologically active substances that appear during allergic inflammation. The effect does not come immediately. It usually takes from 14 days to several months to achieve the effect. These drugs include: Ketotifen, Kromogen, Cromohexane, Nedocromil, Intal and others.
- Antihistamines. They help to eliminate edema from smooth muscle cells of the bronchi. This helps to improve sputum discharge and reduce inflammation. Prescribed by an allergist. Suitable for the control of bronchial asthma: Suprastin, Loratadin, Zirtek, Claritin and others.
- Hormonal. Prescribed for severe asthma, as well as in cases where the previous treatment regimen was ineffective. They have a pronounced anti-inflammatory effect. Long-term use can cause side effects. They can be prescribed in the form of inhalers or in tablets (for severe cases).
For symptomatic treatment and elimination of unfavorable, acutely arisen symptoms of bronchial obstruction, drugs with bronchilitic action are used. They help to quickly eliminate bronchial spasm and improve breathing.
These funds are prescribed as aerosols, which are produced in the form of various inhalers, spacers and nebulizers. They help to distribute the active substance as quickly and efficiently as possible. The smallest particles of the medicine reach the bronchi in the shortest possible time. Usually the effect is achieved within the first 5 minutes from the moment of use.


The following groups of drugs have a bronchodilator effect:
- Adrenomimetics. They block adrenergic receptors, which are located on the surface of bronchial cells. They can be short and extended. Salbutamol-based drugs eliminate bronchial spasm in 5-10 minutes. Foradil, Serevent and Valmax help relieve airway obstruction for 10-12 hours.

- Anticholinergics. They have a pronounced effect. May cause systemic side effects. Blood pressure is often severely reduced. These include: Atropine, Atrovent, Platyphyllin and others.
- Xanthines. Not drugs of choice. They are prescribed only if the previously selected therapy is ineffective. They are often used in combined regimens for the treatment of bronchial asthma. These include: theophyllines, Euphyllin and others.
- Combined. The combination of anticholinergic and adrenergic agonist allows you to achieve a quick effect and keep it for a long time. These include: Berodual, Ditek, Intal plus, Symbicort, Seretid and others. Prescribed for 1-2 inhalations per day. Long-term use may require dose adjustment or replacement with other drugs.
Diet
Nutritional therapy plays an important role in the treatment of bronchial asthma. The diet is of particular importance for the allergic form. In order to prevent the child from having new attacks of the disease, he should follow a hypoallergenic diet regularly. It was developed by the Union of Pediatricians for the treatment of various diseases in which there is a tendency to develop allergic reactions.

Babies suffering from bronchial asthma should completely eliminate highly allergenic foods from their diet. These include:

- Red meats and poultry.
- Tropical fruits.
- Vegetables and fruits in yellow, orange and red colors.
- Seafood and sea fish.
- Citrus.
- Honey.
- Chocolate.
- Sweets and fizzy drinks.
- Manufactured food with a high content of spices, preservatives and colors.
In babies with lactase intolerance, an attack of bronchial asthma may occur after consuming fermented milk products and cow's milk. In such cases, it is better to switch to using goat curd and cheese. These foods will be safer for your asthmatic baby.
The optimal diet for a child with asthma should contain hypoallergenic protein foods, cereals, and enough fiber. Suitable proteins are: chicken breast, rabbit, turkey (if you are not allergic to chicken eggs). For a side dish, you can cook porridge or mashed potatoes or cauliflower.
All cereals can be included in the children's diet. Restrictions can only be made with barley and oatmeal in case of gluten intolerance. Any white and green vegetables and roots are suitable as fiber. Dessert can be apples and pears. Try to choose green varieties grown in the region of residence.


Harbingers of an imminent attack
Before a strong sudden deterioration in well-being begins, the child develops some borderline symptoms. They are also called "aura". Before the development of an asthmatic attack, the child may experience severe sneezing, sore throat, and runny nose.
The baby's anxiety is growing. In some cases, even panic. The behavior of the child may change. He becomes more silent, refuses to make contact. Many children try to be in their own room, as it brings them more peace of mind.
The appearance of a dry cough indicates the transition of the borderline state into a real attack. In the next few hours, all symptoms worsen. A cough begins to increase and numerous dry wheezing appear, and shortness of breath also increases.
After a few hours, the child develops a strong heartbeat and general weakness increases.


Emergency care for an attack
Parents need to know what to do and how to help their baby to successfully manage a sudden deterioration. To do this, use the following tips and an algorithm of actions:

- Do not leave your child alone when the first signs of deterioration appear. An older baby should be asked about what worries him and where it hurts.
- Pay attention to if the child is short of breath. To do this, count the number of breaths in one minute. Assessing this is very simple: observe the movement of the ribs as you breathe. If the number of breaths is more than 20 per minute, then this indicates that the baby has shortness of breath.
- Help your baby get into a comfortable position. Avoid placing your child on their back if breathing is uncomfortable. This situation can only aggravate the development of an attack.
- Provide air flow. If the room is too stuffy, then open a window or window. Try to prevent the child from catching a cold at this time.
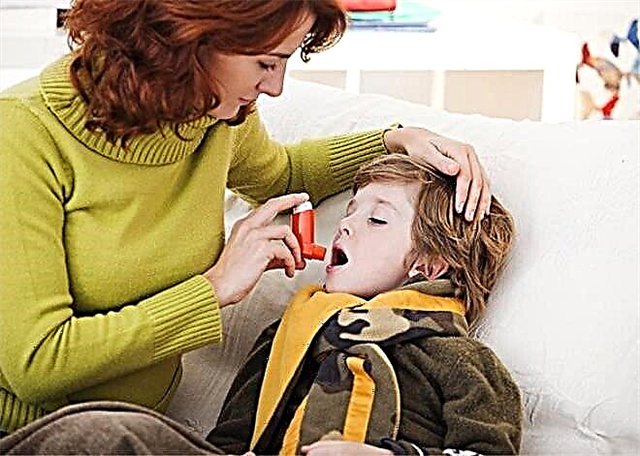
- Use your doctor's recommended inhaler to relieve symptoms. Usually, medications are used to relieve seizures, which have a quick effect. Salbutamol-based inhalers are often used for this.
- If, despite using the medication, the baby continues to have shortness of breath, there is a pronounced cyanosis of the nasolabial triangle and a noticeable decrease in blood pressure, then this is a reason to call an ambulance.
- Do not use 3-4 or more inhalations at a time in an attempt to achieve an effect. Such irrational use can only lead to the development of a dangerous condition that requires hospitalization of the baby in a hospital. Large doses of adrenergic agonists block receptors, which further prevents the bronchi from working fully. To eliminate this effect, intravenous administration of hormones may be required.
Rehabilitation
Carrying out rehabilitation measures in the interictal period will improve the course of the disease, and will also significantly affect the prognosis. If bronchial asthma was registered in a baby for the first time and for a long time proceeded only in a mild course, then competent rehabilitation will help practically lead to recovery, and in some cases even remove the diagnosis.
Rehabilitation measures include:
- breathing exercises;
- massotherapy;
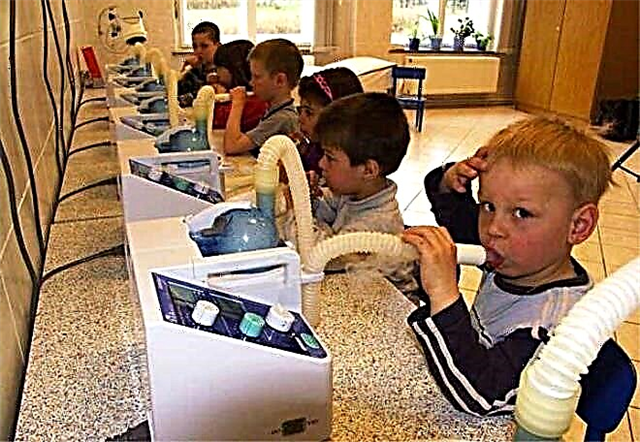
- physiotherapeutic techniques (ultrasound treatment, speleocameras, phonophoresis, hydrotherapy, magnetotherapy, electrophoresis with medicinal bronchodilators, and others);
- Spa treatment;
- a set of therapeutic physical exercises.

All these methods together help to achieve a pronounced therapeutic effect. To achieve a stable remission of bronchial asthma, rehabilitation should be carried out regularly, during the entire period without exacerbations. An individual scheme of rehabilitation measures is drawn up for each baby. Efficiency control is assessed using spirometry and other examinations.

Pulmonary sanatoriums
Strengthening the immune system and sanitizing the bronchi are important components of the basic treatment and rehabilitation of bronchial asthma. Rest with a child in a pulmonary sanatorium will be an excellent option for improving health. You can go on vacation at any time of the year. The choice of a sanatorium should be based on the profile of the services provided.


In Russia, there are many different health resorts that treat and rehabilitate babies with bronchial asthma. Usually they are located in close proximity to the sea or in the beautiful pine forests. The air in such places has a pronounced therapeutic effect on the respiratory system. Vouchers to pulmonary sanatoriums are usually designed for 21 days.
Little patients with disabilities due to bronchial asthma with severe bronchial obstruction can receive free accommodation and treatment in such health centers. Usually vouchers are issued every year. During treatment in a sanatorium, the child's external respiration indicators improve, and immunity is restored.

Prevention
In order for the child not to have new attacks of the disease, a few simple recommendations should be followed:
- Regular use of properly selected inhalers to control seizures.
- Compliance with a hypoallergenic diet.
- Carrying out daily wet cleaning of the children's room.
- Careful selection of bed linen, mattress, pillows and blankets. They should not be made of materials that can cause allergic reactions in the baby.
- Implementation of rehabilitation measures in the interictal period.
- Elimination of all possible allergens from everyday life.
- Regular visits to a pulmonologist and allergist.



