During pregnancy, babies change their position in the uterus many times. As long as the fetus has enough room to move, it can roll over as it suits it best. But from a certain moment, the presentation and posture of the child is important for doctors, because the prognosis for the upcoming birth depends on it. In this material, we will talk about what the transverse position of the fetus is and what to do if the baby decided to sit in the mother's womb in this way.
What it is?
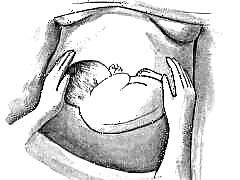
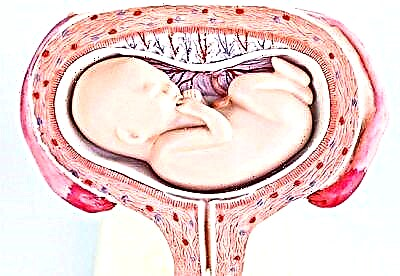
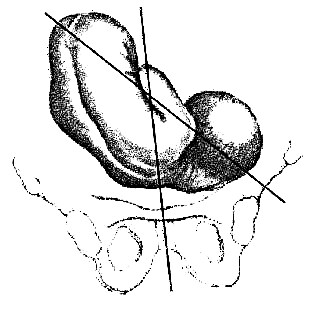
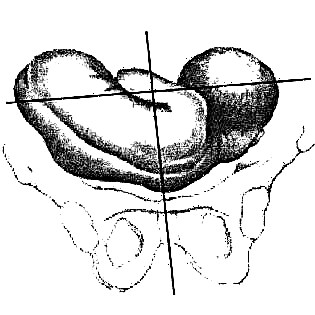
They say about the lateral position when the baby is in the uterus across. If you mentally draw a line along the spine of the child, then in oblique presentation it will intersect with the axis of the uterus at a right angle. In this way, the hip and elbow of the baby can be turned to the exit from the uterus. The head will be located in one side, and the butt in the opposite.
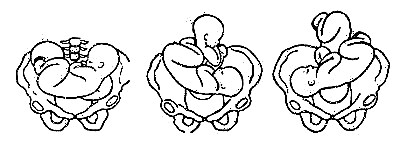
There are several options for the lateral position. If the baby is facing the front abdominal wall of the mother, then we are talking about the transverse facial presentation, if the baby is turned forward with the back, then the transverse position of the fetus with the dorsal presentation is diagnosed. In all cases, a transverse or oblique transverse presentation (if the baby's axis does not create a straight, but an acute angle when crossing with the central axis of the uterus) is considered a pregnancy pathology.
This pathology is rare. Less than 1% of pregnant women are faced with a transverse position of the baby in the womb. In 97% of pregnant women, babies are located in the cephalic presentation, in 2 - 2.5% - in the pelvic presentation. And only in 0.5-0.6% of cases, children accept a transverse presentation, unusual from the point of view of the laws of nature.
Most often, this arrangement of the fetus is typical for women who have given birth a lot and often. In the first pregnancy, transverse presentation - isolated cases. Until 34-35 weeks of pregnancy, there is no talk of pathology, because the baby has practical and theoretical opportunities for an independent turnover in the uterus for childbirth, but after 35 weeks, the turnover becomes almost impossible, because there is no free space for such wide movements in the uterus

Dangers and risks
This situation does not significantly affect the course of pregnancy itself. However, it should be remembered that any abnormal position of the baby in the uterus is a significant risk factor for premature birth. In the case of the transverse position, this happens in 40% of cases. A child who will be born much earlier than the intended obstetric term cannot always adapt to a new environment for himself. So, with immaturity of the lung tissue, problems with spontaneous breathing may arise, acute respiratory failure may develop, and with a low weight of a child born prematurely, it will be difficult for the baby to keep warm.
In the case of the onset of spontaneous childbirth, small parts of the body and umbilical cord loops may fall out along with the outpouring of water. This is fraught with the death of the child, injuries, deformities, disability, the development of severe complications from acute hypoxia. For a woman, such childbirth is dangerous with injuries to the pelvic bones, ruptures of the perineum, cervix and body of the uterus, vagina, and heavy bleeding. In severe cases, everything can end in the death of both the child and the woman in labor.
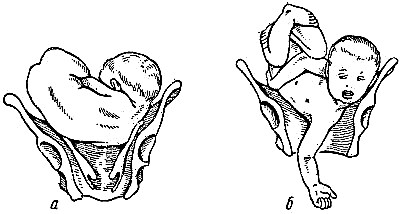
With rapid spontaneous childbirth, the shoulder of the child is often "hammered" into the small pelvis, this is how the neglected lateral position of the fetus develops, in which spontaneous childbirth is impossible. It is when the transverse position is neglected that the traumatic rupture of the uterus most often occurs.
If the position of the child is oblique, then it is considered transitional. Theoretically, even in childbirth, it can change either longitudinal or transverse. Naturally, no one will wait until the baby turns, the risks are too high.
That is why, with transverse presentation, it is recommended to give birth by surgical intervention - a cesarean section allows you to remove the child from their womb without the risk of severe birth trauma, hypoxia. For the expectant mother, the operation will also guarantee that her small pelvis and perineum will not suffer from ruptures and fractures.

Causes
Most often, babies find themselves in a transverse position, for whom it is easy and free to move in the uterus, even for long periods. This physical activity is promoted by polyhydramnios. If the amount of amniotic fluid is higher than normal, then the baby may well take this position and "get stuck" in it. Also, active movements for long periods are facilitated by weak and overstretched walls of the uterus. Weakness and some flabbiness of smooth muscles are characteristic of women who give birth a lot and often.
No matter how strange it sounds, the lateral position is also promoted by low physical activity, or rather, the inability for the child to move. This condition is characteristic of lack of water. Also, large hypertrophied children experience difficulties with movements and coups.
The risk of transverse presentation of one of the children or both at once is in a woman with multiple pregnancies, which is why the position and condition of each of the fetuses is closely monitored throughout the entire multiple pregnancy.
The baby can take a lateral position as the only convenient one if a woman almost constantly has an increased uterine tone during pregnancy, and also has tumors or other neoplasms in the lower uterine segment. The establishment of a normal head presentation, because of this, becomes unacceptable for the child. In addition, transverse or oblique presentation is often observed during pregnancy in women with congenital abnormalities of the main reproductive organ - a saddle or two-horned uterus.
Quite often, the placenta interferes with the baby, if it is located low, they have its full or partial presentation. When the entrance to the small pelvis is blocked by something, the baby cannot stand in the correct posture - head presentation. A child in a woman with a clinically narrow pelvis can also sit across the womb.
Sometimes the reason for the wrong position of the child lies not in maternal factors, but in the child itself. So, with hydrocephalus (dropsy of the brain) or anencephaly (absence of the brain), the baby does not take a head position, but remains either sitting in a breech position or lying across the uterine cavity.
Diagnostics
A transverse presentation can be determined by an obstetrician-gynecologist during an external examination of a pregnant woman, as well as during a vaginal examination. Usually, the height of the standing of the fundus of the uterus, which is measured at each planned appointment in consultation, with a transverse position is below normal, and the pregnant tummy itself even visually looks like a torpedo melon. On palpation, the position of the fetus is determined by the location of the head - this is the hardest and most mobile part of the child's body. With a cephalic presentation, it is felt in the lower abdomen, above the pubis, with a pelvic presentation - near the bottom of the uterus (in the upper abdomen), with a transverse presentation, the head is either in the right or in the left side of the expectant mother.
The baby's heartbeat is determined near the belly button of the expectant mother. Vaginal examination allows to exclude presentation of the head or priests. Then the expectant mother is recommended to undergo an ultrasound scan. Only ultrasound scanning allows you to get the most accurate data about the position of the child, what are the features of his position, which part of the body is located towards the exit to the small pelvis, and also to assume the weight of the baby. All these data are needed so that the doctor can more carefully assess the risks and choose the right delivery tactics, in which neither the mother nor the child will suffer.

What to do?
If a woman has a transverse presentation at 24-25 weeks of pregnancy, as well as earlier or later than this period, there is no need to panic. Up to 35 weeks, the baby has time for a coup. The expectant mother needs to try with all her might to help her child to take the correct position in the uterine cavity.
For this, special gymnastics is recommended, in which each exercise is thought out in such a way as to relax the muscles of the uterus as much as possible, to give the baby the opportunity to turn. The set of exercises includes exercise complexes of Dikan, Shuleshova, Grishchenko. There are other complexes developed by gynecologists specifically for women who need help turning their baby around. It should be noted that with a positive attitude and daily exercises, the effectiveness of gymnastics reaches about 70-75%. It is this percentage of babies that nevertheless go from an unstable transverse or oblique arrangement to a head one.
Fetal flip exercises are not recommended for everyone. So, it is forbidden to do exercises for women suffering from diseases of the heart and blood vessels, kidneys, and liver. A scar or several scars on the uterus from a previous cesarean section or other surgical operations are also a contraindication.
If a pregnant woman has edema, signs of preeclampsia, the threat of termination of pregnancy, spotting, presentation or a low location of the placenta, gymnastics cannot be done.
It is advisable to do gymnastics for those for whom it is not contraindicated from 30 to 36 weeks of pregnancy. If the baby stubbornly does not want to accept a different position, doctors can offer an obstetric coup according to Arkhangelsk. It is done in a hospital under ultrasound control. The kid is deployed manually. But such an intervention is quite dangerous, it can provoke rupture of the membranes, the outpouring of amniotic fluid, the onset of premature birth, as well as injury to the fetus. That is why doctors themselves rarely decide on an obstetric turn.
Separately, I would like to emphasize the importance of a positive attitude of a pregnant woman. Many experts claim that the methods of persuading the baby, gentle persuasion, combined with corrective gymnastics, give amazing results.
If the expectant mother herself is in the mood for the best, will remain calm, harmonious mood, then the chances of her baby for an independent coup closer to childbirth will significantly increase.
With transverse presentation, it is important to prevent premature birth. That is why a woman should be extremely careful not to lift weights, do not jump, do not make sharp bends of the body.
Care should be taken to have sex, because an orgasm and even the usual sexual arousal in a woman cause short-term spasms of the smooth muscles of the uterus. If, simultaneously with the transverse presentation, a low position or placenta previa is diagnosed, then it is recommended to refuse sex altogether, as well as from masturbation. Stress should be avoided.
Additionally, a woman should wish only on her side, completely repeating the pose of her baby. How to do this correctly, the doctor will tell you after the ultrasound scan, since he will see the exact location of the child's body and body parts.
You can not miss scheduled visits to the doctor in the antenatal clinic. Most likely, the attending doctor will suggest early hospitalization - at 36-37 weeks of pregnancy, and this will be the only reasonable solution to avoid unwanted complications. In no case should you refuse it.

If, despite all the precautions, the woman began to deliver prematurely, regular painful contractions appeared, the water receded, it is important to take a horizontal position in order to prevent the baby's handle from falling out of the genital opening, which is in breech presentation. After that, you need to immediately call an ambulance.
The woman will receive emergency care, with a 99% probability she will undergo an emergency caesarean section immediately after she is delivered to the hospital.
Can I give birth on my own?
Childbirth with a transverse presentation can be dangerous, we talked about this above. With this position of the baby, in 99% of cases, a cesarean section is performed. It is better if it is carried out before the onset of spontaneous labor, which is why early admission to the hospital is recommended.
Absolute indications for surgery are post-term pregnancy in a transverse or oblique presentation, fetal hypoxia, and the presence of scars on the uterus. If the pregnant woman was taken to the hospital on an "ambulance" with the discharge of water, doctors will make sure that the parts of the child's body have not fallen out. If a prolapse is found, it is forbidden to set the handle or umbilical cord back.


If, by the time of hospitalization, the woman's cervix is fully disclosed, doctors may try to turn the baby on its leg, so that it can then be removed with its legs forward. But they will not always do this, but only if the baby is very premature, weighs little, and also during pregnancy with twins, if one of the babies lies across.
If the anhydrous period (the time elapsed since the discharge of water) is delayed, then the likelihood of infection of the uterine cavity and the development of fetal hypoxia increases. The critical time is considered to be 12 hours.
If a woman is brought to the ambulance after a long anhydrous period, a cesarean section will be performed in any case, regardless of the degree of cervical dilatation.

Late treatment is life-threatening for a woman with sepsis. Often in such situations, after a cesarean section, you have to perform another operation - a hysterectomy (complete total removal of the uterus). A woman will never be able to become a mother.
Given the high risks, a planned cesarean section at 37-38 or 38-39 weeks of pregnancy looks like a more reasonable way out of the situation. The operation takes about 40 minutes, and after 10-12 hours the woman will be able to get up. Modern methods of anesthesia allow the expectant mother to be conscious during the removal of the crumbs and not feel pain at the same time, and therefore, as in natural childbirth, she will immediately be able to look at her son or daughter, the baby will be immediately attached to the breast.


Reviews
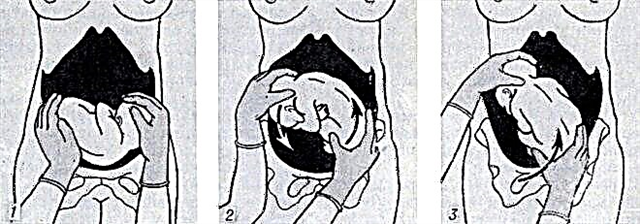
Expectant mothers who have left their comments on thematic forums claim that the folk method of stroking the abdomen is very effective for turning the baby from the transverse presentation. They recommend several times a day, or better every free minute, stroking the stomach with your right hand clockwise. For some, according to reviews, these simple manipulations helped and the babies were able to turn into a normal natural position, the birth took place without complications.
Cases are also described when babies made a long-awaited turn almost a couple of days before the planned caesarean section, and the doctors changed the delivery tactics in favor of natural childbirth.

True, in the case of transverse presentation, it is quite difficult to predict which direction the baby will turn in. Therefore, some women described their experience - the baby turned to the pelvic position. The operation in this case was also carried out as planned.
According to the reviews of pregnant women who managed to "turn" their baby from a lateral position in the womb, swimming and water aerobics help in this, especially exercises in which the mother takes a position upside down. However, such techniques should only be used under the supervision of an experienced trainer or physician.
Cases of natural childbirth with preserved transverse or oblique presentation on the forums of expectant mothers have not been described, since they are extremely rare and not always successful.


For the position and presentation of the fetus, see the following video.