Women in preparation for childbirth can face a host of previously unfamiliar medical terms. One of them is epiziorrhaphy. In this article we will tell you what this procedure is, how it is carried out and why. This will help women better understand the birth process and be more prepared for it.
What it is?
Epiziorrhaphia is a compound medical term Episiorrhaphia, which, according to the 2000 edition of the Comprehensive Medical Dictionary, contains two concepts: "Episio" is translated from Greek as "female external genital organs", and rhaphe is "seam". Thus, it is easy to guess what this term means surgical manipulation of stitching a dissected female perineum.
The dissection itself is called an episiotomy. Such an operation can be performed during childbirth if the prerequisites arise that allow the doctor to be sure that without dissection, a spontaneous rupture of the perineum can occur, in which not only the genital tract, but also the urinary tract, as well as the rectum and anus can be injured.
During childbirth, it is very difficult to calculate anything in advance, and therefore an episiotomy may be needed at any time of the second stage of labor, when there are attempts and there are difficulties with the birth of the head or shoulder girdle of the fetus. The incision, made in a certain way (one of the existing ones), allows you to expand the perineum to such a size that the baby can be born without getting serious birth trauma.
When is it held?
Episiotomy, as you might guess, will be used when there is a need to suture the incision made during the episiotomy. At the same time, sutures are started only after the complete completion of labor, which, as you know, ends with the birth of the placenta.
If the afterbirth that has come out does not inspire fear in the doctor, there is no reason to assume that its fragments remain in the uterus and that there are cervical ruptures, preparation for episiorrhaphy begins. In all other cases, first eliminate the existing problem. In any case, epiziorrhaphy is the final "stroke", after its implementation, the birth is considered completely completed.
Since the incision can be made either perpendicular to the anus (perrineotomy) or laterally at a 45-degree angle at least 2.5 centimeters away from the anus (midline or lateral episiotomy), the incision will be sutured in different directions.
The doctor's task is to dock the edges of the wound as accurately as possible and restore their integrity, thereby reducing blood loss and the likelihood of infection entering the wound.

Execution technique
When starting an epiziorrhaphy, a healthcare professional first treats his own hands with an antiseptic. The woman's perineum is treated with an alcoholic solution of chlorhexidine. This solution is optimal in this case, since it reliably disinfects and does not cause an alcohol burn.
The physician puts on sterile gloves, prepares gauze balls for blotting during the suture process. Then proceed to pain relief. Even if they cut, as women say, "profit", then the crotch will be sutured with anesthesia. Today, the Ministry of Health recommends that the incision also be anesthetized, but most obstetricians are sure that the moment of the incision, which is carried out at the very peak of the next attempt with one movement of the surgical scissors, is generally not felt by the woman.
There are two ways to relieve anesthesia after an episiotomy.
- Infiltration anesthesia implies the introduction of anesthetic (more often "Lidocaine") directly into the tissue to be sewn.
- Pudendal anesthesia involves the introduction of novocaine or another anesthetic into the pudendal nerve, located about a centimeter proximal to the sciatic bone. The anesthetic can be administered both through the walls of the vagina and through the perineum.
In both cases, the woman remains conscious, she simply does not feel acute pain during manipulation. General intravenous anesthesia can only be given if there is a need to remove the placenta manually, suture the cervix in case of ruptures. In this case, the final part of the epiziorrhaphy manipulations does not require a separate anesthesia. While the woman is sleeping, they will have time to put all the necessary stitches on her.
If during childbirth the woman was given an epidural, nothing would be required to inject into the perineum at all; if necessary, the anesthesiologist will introduce an additional dose of anesthetic into the catheter installed in the spinal canal.
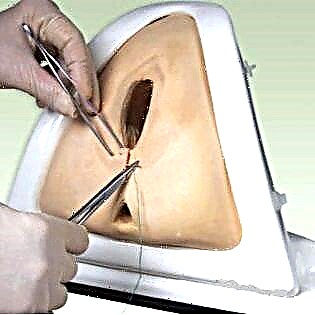
Only a sterile set of instruments is used for suturing.
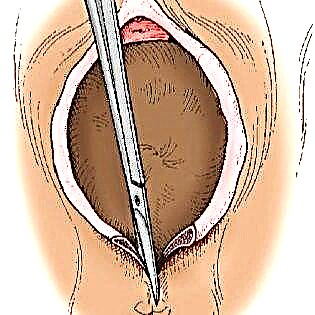
Suturing begins with the damaged mucous membrane of the posterior wall of the vagina. The first suture is applied from the top of the incision sequentially downward. Then the vaginal wall is sutured with catgut from top to bottom in the same direction.
It is customary to suture the muscles of the pelvic floor with catgut. Dip sutures are used along the edges of the dissected muscles. The skin is sutured last - for this suture material such as vicryl sutures can be used. You can also make a seam cosmetic, located actually intradermally. After finishing the suturing, the area is treated with an antiseptic again.
The suture technique can vary.
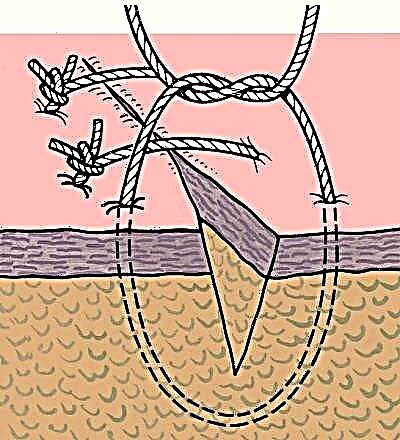
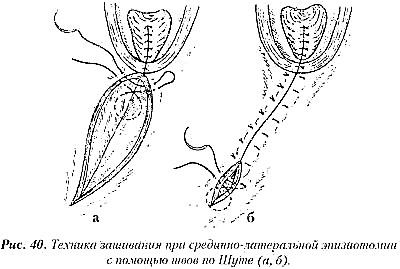
Often, doctors use Shute's perioneorrhaphy, when all layers of dissected tissues are immediately fastened with sutures resembling eights. The method is quite quick, but, alas, not without reproach - the Shute sutures must be removed, since the technique does not imply self-absorbable materials. Also, such sutures are more likely to become infected in the early postpartum period. Layer-by-layer suturing is considered more preferable today.
How the suture will heal after childbirth depends on what the material will be, what technique of suturing the doctor will use.
Possible complications
The perineum is not the most convenient place for sterile dressing and stitching. In addition, the place of suturing comes into contact with abundant secretions - lochia. The blood mass can become a breeding ground for pathogenic bacteria, and then the suture can become infected, disperse, heal for a long time or form with an anatomical defect.
To avoid such complications after episiotomy and episiorrhaphy, following the recommendations will help:
the seams are daily treated with brilliant green, "aired";
a sanitary napkin or underlay is used only sterile in the first 2-3 days after childbirth, changed at least once every 2 hours;
you need to wash yourself after each bowel movement or urination;
for 2-3 weeks, you should sit only with support on one thigh - from the side opposite to the incision line, feed the child and eat yourself either lying down or standing;
sutures usually heal within a week, after which they can be removed if they are sewn with silk threads;
after discharge from the hospital, you need to continue to process the seams with brilliant green;
constipation and other situations in which a woman will have to over-strain the perineum should not be allowed.
If you find problems with sutures, be sure to contact a gynecologist, since most of them require treatment.